
DSI Student Peter Dupont Grantcharov is Lead Author of the Data-driven Study
Peter Dupont Grantcharov, Master of Science candidate, Columbia University Data Science Institute.
A new study reveals that during stressful moments in the operating room, surgeons make up to 66 percent more mistakes on patients. Using a technology that captured the electrical activity of a surgeon’s heart, researchers found that during intervals of short-term stress, which can be triggered by a negative thought or a loud noise in the operating room, surgeons are much more prone to make mistakes that can cause bleeding, torn tissue, or burns.
The results of the study, published in the open branch of the British Journal of Surgery, could lead to the development of protocol aiming to reduce acute or short-term stress on surgeons working in the operating room. Medical errors cause between 250,000-440,000 deaths annually in the U.S., with a proportion of those mistakes occurring in operating rooms. Any change in common practice that reduces the number mistakes made by surgeons due to stress would also reduce the number deaths.
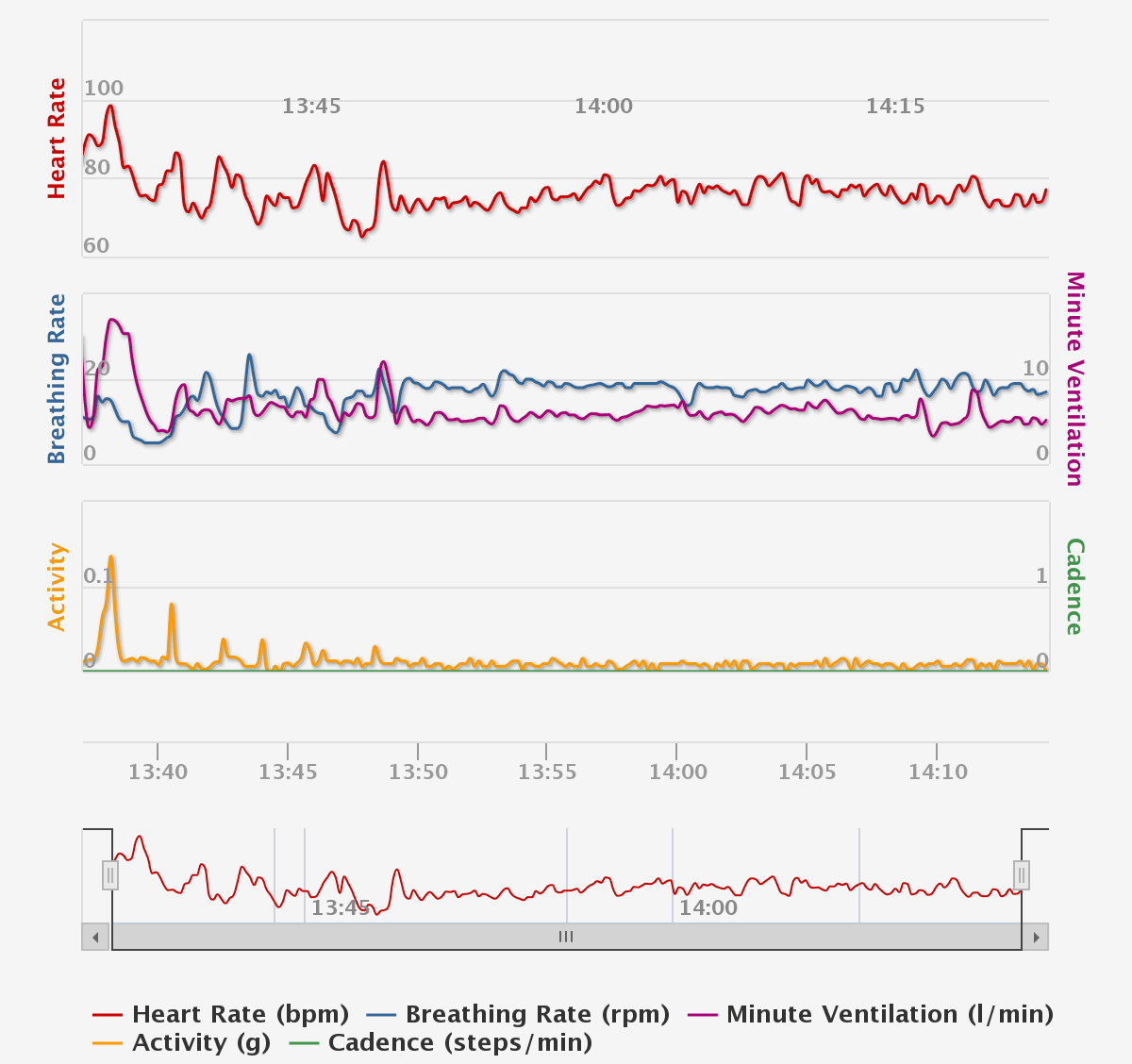
It’s an important study published in a prestigious journal, and even more impressive is that its lead author, Peter Dupont Grantcharov, is a master’s student at the Data Science Institute at Columbia. A year and a half ago, Grantcharov had the idea to ask Dr. Homero Rivas, Associate Professor of Surgery at Stanford Medical Center, to wear a Hexoskin Smart Shirt under his scrubs while he did surgeries. The shirt, designed to give athletes precise physiological data during workouts, measures the electrical impulses that trigger heartbeats. From this data, Grantcharov derived heart-rate variability statistics ‒ the variation in times between heartbeats, to determine Rivas’s momentary stress levels.
Grantcharov was also allowed in the operating room, where he collected laparoscopic video recordings of Rivas as he worked. Another researcher later reviewed the recordings and documented Rivas’s mistakes using validated frameworks for assessing surgical performance. Both his stress levels and surgical errors were time stamped so that Grantcharov could correlate the two. This data yielded the somewhat alarming finding that the effect of short-term stress on surgical error is as high as a 66 percent increase.
“I was surprised by that, as well as by the amount of distractions in the operating room,” says Grantcharov, who did the study while working as a research assistant at the Stanford Medical Center before enrolling at DSI. “Many machines have alarms that go off periodically, equipment malfunctions, side conversations take place, people walk in and out of the OR – I could go on. My hope is that other researchers will build upon our work to make further strides in learning about the causes of stress on surgical personnel. If our study helps make the OR a safer place for patients, I’d be thrilled.”
Grantcharov was involved in designing the study, collecting and analyzing the stress and surgical performance data as well as writing the manuscript. It was his first experience with data science, and he loved it. In point of fact, this research is what prompted him to enroll in the master’s program at DSI, where he’s now in his first semester.
In this Q&A, Grantcharov talks in detail about how he conducted the study and wrote the paper, as well as his hopes for the outcomes of the research.
How’d you get the idea for this study?
I had read several papers that had studied the relationship between stress and surgical performance, but only in virtual surgical environments. At the time, there wasn’t a technology that allowed for researchers to unobtrusively study surgeons at work in the OR. Getting continuous ECG readings was simply too obtrusive to implement in a live surgical setting, as even the smallest impediment in the surgeon’s ability to perform his or her job would be unacceptable for research. This presented obvious limitations in being able to reveal insights of how stress affects surgeon. I did this study during my second summer working as a research assistant at the Stanford Medical Center. At the time, I was a pre-med undergraduate student majoring in life sciences and statistics at Queen’s University in Kingston, Canada. This was a great project in which I was able to apply elements from both fields, and it was a topic I was immensely curious about exploring.
 Researchers in other fields have studied the relationship between stress and performance, haven’t they?
Researchers in other fields have studied the relationship between stress and performance, haven’t they?

Several high-performance industries, notably aviation and professional sports, have investigated the relationship between stress and performance. There is agreement that some stress can be beneficial because it leads to heightened focus, but too much stress, especially for complex tasks, is widely accepted to be detrimental. This research has been responsible for causing protocol changes to reduce stress exposure, notably for pilots in the aviation industry, along with training initiatives to help professionals cope with stress. I saw no reason why we shouldn’t strive to have the same level of understanding of how stress impacts another high-performance domain: surgery.
How’d you hear about the Hexoskin shirt and come up with the idea to use it in the OR?
I was researching ECG monitors and came across the shirt. It was clear that it was a perfect fit for the objectives of the study, given its precise technology, and even more importantly, its unobtrusiveness. The shirt functions not dissimilarly from a lie detector test – that is to say by revealing insights to physiological states that are not visually apparent. In this case, by taking 256 electrocardiogram (ECG) measurements per second with three sensors. Stress triggers could have been something as simple as a thought that came into the surgeon’s head, or something more conspicuous and identifiable like an alarm/phone going off, or distracting background communication. The heart rate variability data would indicate that the stress response had been triggered if there was a response from the surgeon to these potential triggers. We did not attempt to draw any conclusions regarding the possible triggers of stress for this study – it was only postulated and is the next logical step for future research.
Can you discuss how you framed this project?
After designing the study, it was definitely critical to assemble the right team to bring it to fruition. To start, I cannot even begin to express my gratitude to my supervisor, Dr. Rivas, for giving me the autonomy to carry out this study as I had envisioned, particularly because of its impact potential and somewhat controversial nature. No one enjoys being observed and critiqued, so his honesty, integrity, and commitment to the advancement of knowledge in this important domain were evident.
Conducting the study was a team effort. I had invaluable assistance and consultation from computer science post-doc Thomas Boillat and Katarzyna Wac, associate professor of computer science, both of whom are co-authors. They were instrumental in getting the data analytics for this project underway. It was a bit intimidating at the onset for a pre-med student like me to handle several hundred thousand data points, so their assistance was key. So while I oversaw every step from inception to manuscript completion, occasionally spending upwards of 12 hours a day in the OR collecting data, the study wouldn’t have gotten off the ground without the team.

(from left to right) Sharon Wulfovich, MD candidate, UC San Diego School of Medicine; Dr. Katarzyna Wac, Associate Professor of Computer Science at University of Copenhagen; Dr. Homero Rivas, Professor of Surgery at the Mohammed Bin Rashid University of Medicine and Health Sciences; Peter Dupont Grantcharov, Master of Science candidate, Columbia University Data Science Institute.
What was it like in the OR?
It was a phenomenal experience. Before going to Stanford, the only OR experience I had was from watching television on my couch. Performing a successful surgery calls for an intricate team effort that has to function like a well-oiled machine. That said, given that I was trying to observe short-term stress by the surgeon, I didn’t have a hard time identifying stressors, which was a bit surprising.
How’d you become a research assistant at Stanford and were you prepared for it?
I met Dr. Rivas at a conference about wearable technology in healthcare. When you’re an undergraduate student trying to survive winters in Canada, your eyes light up when you hear the words: Palo Alto, California. When the research assistantship opened up, I applied and got it. As the study was transpiring, it became evident that I’d needed computer science skills for data analytics, so I took an online course to develop my coding skills. By the end, I learned enough to write most of the scripts and manage the data for this research. It was a long project; it took more than a year from inception to publication. I’m proud that the paper is published. It’s been quite the journey, to say the least.
Can you talk about how you captured the data and analyzed it?
The frameworks for 1) how to objectively measure stress and 2) how to objectively assess surgical performance had already been established and validated. So for me, the major obstacle was figuring out a way to apply this knowledge to develop a method that made sense in the context of what we were studying. The Hexoskin ECG data was directly available in CSV form, which was ideal, so to translate this into stress data I had to write a program that was able to calculate the required heart rate variability statistics over different time intervals. If you have ever seen the ECG monitor beeping in movies, these HRV statistics essentially observe how much variation there is in the time between the sharp peaks you’d see on those graphs. When an individual is stressed, the sympathetic nervous system (i.e. the fight-or-flight system) takes charge and makes the intervals between these peaks incredibly consistent. When relaxed, there is much more variation. It’s a remarkable phenomenon. These statistics were calculated over discrete time intervals, and were then juxtaposed on a single timeline with the surgical performance data, to allow us directly observe any association between the two variables.
How many surgeries did you observe?
In total, we captured data for 25 surgical procedures. This included gastric bypasses (12 patients), sleeve gastrectomies (7) and peroral endoscopic myotomies (6), with a mean duration of 96.7 minutes for all procedures.
What are the most important findings from your research?
Even more so than studying how stress and surgical performance relate, the primary objective of our study was to serve as a benchmark for future research aiming to study how stress impacts surgical performance. We hope that other researchers will build upon the methods we showed to be effective, and proceed to look into triggers that cause elevated stress; when we learn about these triggers, it’ll be critical to investigate how to manage the ones which we have control over. A primary culprit, I speculate, will be distractions in the OR, like I mentioned earlier. If those distractions can be identified, and steps taken to mitigate or eliminate them, operating rooms would be much safer for all of us.
The results of your study are impressive, but somewhat worrisome. Has your paper had any effect on how to improve stress in ORs?
It’s a new study; it will take time. But that such a prestigious journal published it is a great sign. Personally, I feel we took a great leap in developing sound methods in studying the relationship between stress and surgical performance. That the actual results were so revelatory was a bonus for an exploratory study like this. It’s important to note that we did not study the potential stressors that could have affected the surgeon’s stress level and ultimately his performance, we solely focused on the association between the observed stress levels and surgical performance.
You’ve said that doing this study motivated you to study data science. How so?
Doing this research was my first exposure to using data science techniques to learn truths that are inaccessible without large datasets. I liked the work and perhaps felt that I had an aptitude for it. This study was also occurring at a time that I was having second thoughts about medical school, so it was an organic way for me to transition from medicine to data science. Plus, I had always been a math nerd at heart, and this study showed me that being a doctor is not the only way to help people. Data science will perhaps allow me help people on an even greater scale.
What do you plan to do after you get your master’s from DSI? Stay in the medical field?
Applying data analytics to positively impact healthcare would be incredibly fulfilling and that is certainly something that motivates me. But with that said, I learned my lesson from being too committed to one path as a pre-med. That is perhaps the quality I love the most about data science – it can applied to anything and everything. So at this point, I’m open to any opportunities that present themselves.
— Robert Florida